
Kaiser Permanente strikers have a point
Healthcare workforce shortages are bad — here’s what can help

While the decades-long U.S. political focus on expanding insurance coverage helped bring the uninsured rate to an all-time low of 8 percent last year, policymakers haven’t paid enough attention to the other side of the ledger: the supply of healthcare providers available to care for patients.
The latest figures indicate that the number of job openings in the health care and social assistance sector exceeded 1.75 million in August, two-and-a-half times higher than a decade earlier. While shortages have eased since their peak in 2022, job openings remain far above pre-pandemic levels.
Job Openings in the Health Care and Social Assistance Sector, U.S. Total
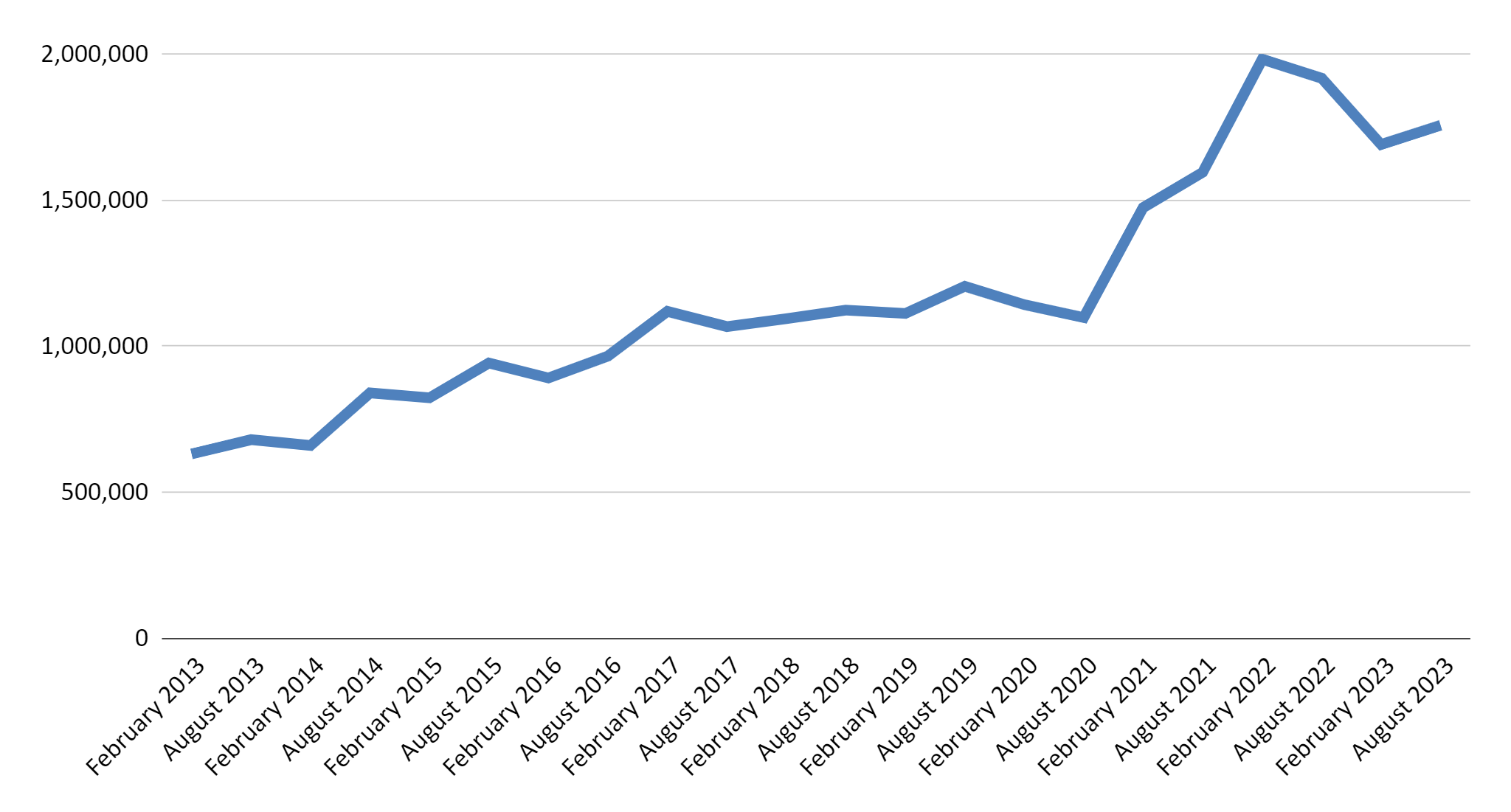
Source: U.S. Bureau of Labor Statistics, Job Openings and Labor Turnover Survey
Last year, the Health Resources and Services Administration estimated that nearly 100 million Americans lived in areas with shortages of primary healthcare professionals. Shortages of mental health providers are even more acute, affecting 156 million people. Unsurprisingly, residents of shortage areas report being in worse health and having greater difficulty getting care.
Even when patients in shortage areas are able to overcome long wait times and see a provider, they often receive subpar care. Understaffing in hospitals and nursing homes has consistently been associated with worse outcomes, including higher mortality rates and more medical errors. In some areas, increasing the density of primary care providers could substantially improve life expectancy.
Chronic worker shortages set in motion a vicious cycle where understaffed facilities place additional burdens on the shrinking number of existing providers, leading to burnout and fueling even deeper shortages. Not only that, but those considering a career in healthcare may be deterred by the prospect of poor working conditions. When 75,000 Kaiser Permanente workers launched the largest healthcare industry strike in U.S. history last week, the short-staffing crisis was their top grievance.
And for good reason. If current trends continue, the gap between the demand for healthcare services and the number of trained providers will widen into a chasm. One analysis estimated that “the number of states receiving a grade of “D” or “F” for their physician shortage ratio will increase from 4 in 2017 to 23 by 2030, with a total national deficit of 139,160 physician jobs.” Even before the pandemic, a 2019 paper found that up to 1.2 million new nurses would be needed by 2030 to meet recommended staffing levels.
Reversing these trends requires swift action by federal and state policymakers.
Relax immigration restrictions that prevent well-qualified foreign healthcare workers from entering the U.S. The H-1B temporary work visa is the primary pathway for high-skilled foreign professionals to enter the country. But since 2004, the federal government has imposed an arbitrary cap on the number of H-1B visas available, limiting the ability of health care facilities to fill critical vacancies.
Expand scope-of-practice and embrace new types of providers. Barely half of states grant nurse practitioners full practice authority, despite a substantial body of evidence that allowing nurse practitioners to work independently improves access to care without harming patients. As another example, only 13 states permit dental therapists, mid-level providers who can perform basic preventive and restorative services. Removing unnecessary regulatory barriers like these could help alleviate dire shortages of dental care in rural America.
Remove barriers to direct primary care. One of the biggest reasons physicians are leaving the profession — and young people are thinking twice about pursuing careers in medicine — is the growing burden of administrative tasks that detract from the doctor-patient relationship. One study found that office-based physicians spend just 27% of their total time on direct clinical face time with patients and nearly half of their time on paperwork, much of it tied to insurance billing. By rejecting third-party payment, doctors in direct primary care are able to focus their energy on what they care most about – patients – and are less likely to burn out.