
Minimum-Staff Requirements Will Help Some Nursing Home Residents; Payment and Regulatory Reform Would Do More

The Centers for Medicare and Medicaid services recently announced a new minimum staff requirement for nursing homes. The goal behind the requirement is to improve the quality of long-term care, which happens to be a question I’ve researched a lot, so in this post I want to add some commentary to what Grabowski and Bowblis, two of the field’s leading experts, wrote in a recent piece in the New England Journal of Medicine, where they called the new rule possibly the “most important nursing home reform in decades.”
First of all, what is the rule proposing? The rule would require minimum staffing levels in nursing homes of 0.55 hours-per-resident-day (HRPD) for Registered Nurses (RN’s) and 2.45 HRPD for Certified Nursing Assistants (CNA’s). Notably, the rule does not propose a minimum for Licensed Practical Nurses (LPN’s), but CMS indicates they’re also considering an overall minimum of 3.48 HRPD. The rule would be phased in over 2-3 years and there are some funds to help nursing homes train/attract workers ($75 million to be precise), but it’s the staff requirements that are potentially a big deal.
For readers unfamiliar with the area, it's a commonly held view among scholars that nursing homes are chronically understaffed, and that this is a major contributor to the troubling health outcomes we often observe. For instance, 1 in 10 residents develop bedsores, even though bedsores are preventable by shifting a resident’s position on an hourly basis and other well known but typically labor intensive protocols.
Back to the proposed rule. In column 3 of the table below, Grabowski and Bowblis show that only 19% of facilities currently meet both the RN and CNA requirements, which means a striking 81% would either have to hire more nurses and nursing assistants, and/or admit fewer residents, to comply with the proposed rule.

Grabowski and Bowblis are favorably inclined toward the CMS rule, even though they are well aware and point to many of the unintended consequences likely to occur. Tellingly they write:
Levels of nursing staff are a symptom, rather than the root cause of the problem. Staffing levels are a function of a broader set of system-level challenges related to how the United States pays for and regulates nursing home care.
In my own work I’ve studied the worst performing nursing homes — places that have chronically failed their patients for three, five, sometimes even 10 years, and that you may have heard about in the news for all the wrong reasons.
A paper that I’m currently revising shows there’s an upside: When payments and oversight become more closely tied to the outcomes of residents, even the worst facilities respond to those incentives. As a sneak-peak to this forthcoming paper, I show below that if we tie financial performance to patient outcomes, high risk residents suffer fewer bedsores.
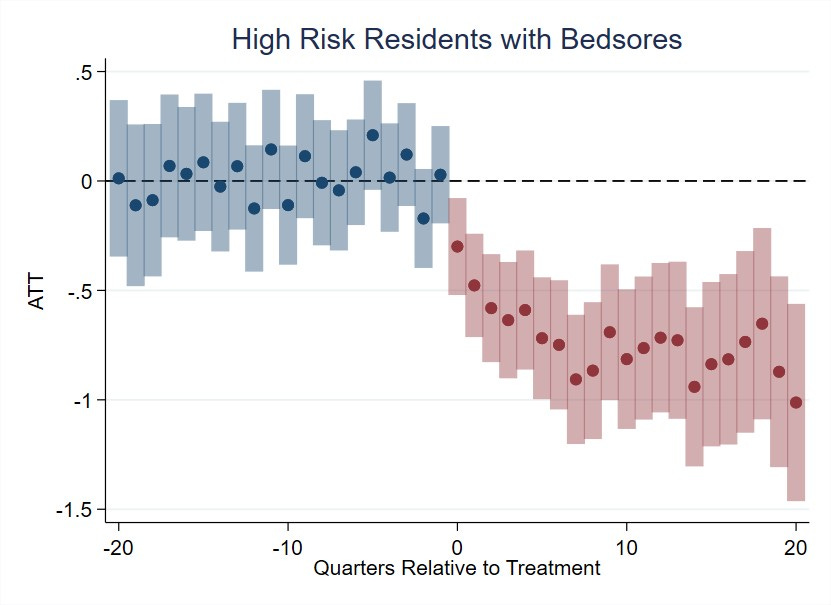
The graph below shows this is partly due to more nursing staff. The crucial point, however, is that more staff is not the only way or necessarily the best way to achieve better outcomes. As Doug Holz Eakin once put it, “Programs should strive to pay for outcomes and let participants find the inputs [..] that achieve those outcomes at least cost.”
More staff will help nursing home residents, but to improve lives at the lowest possible cost we need fundamental regulatory and payment reforms.
