
Best of Open Health: Medicare Spending - Physician Services Are a Much Bigger Problem than Drug Prices
Healthcare spending will continue to spiral out of control unless we change how we pay for physician services.

Note [M.B.]: A recent post made the point that Medicaid spent about twice as much on improper payments than on prescription drugs in 2022. This week we follow up on that theme by reposting Elise Amez-Droz excellent post on physician services and drug prices. Enjoy!
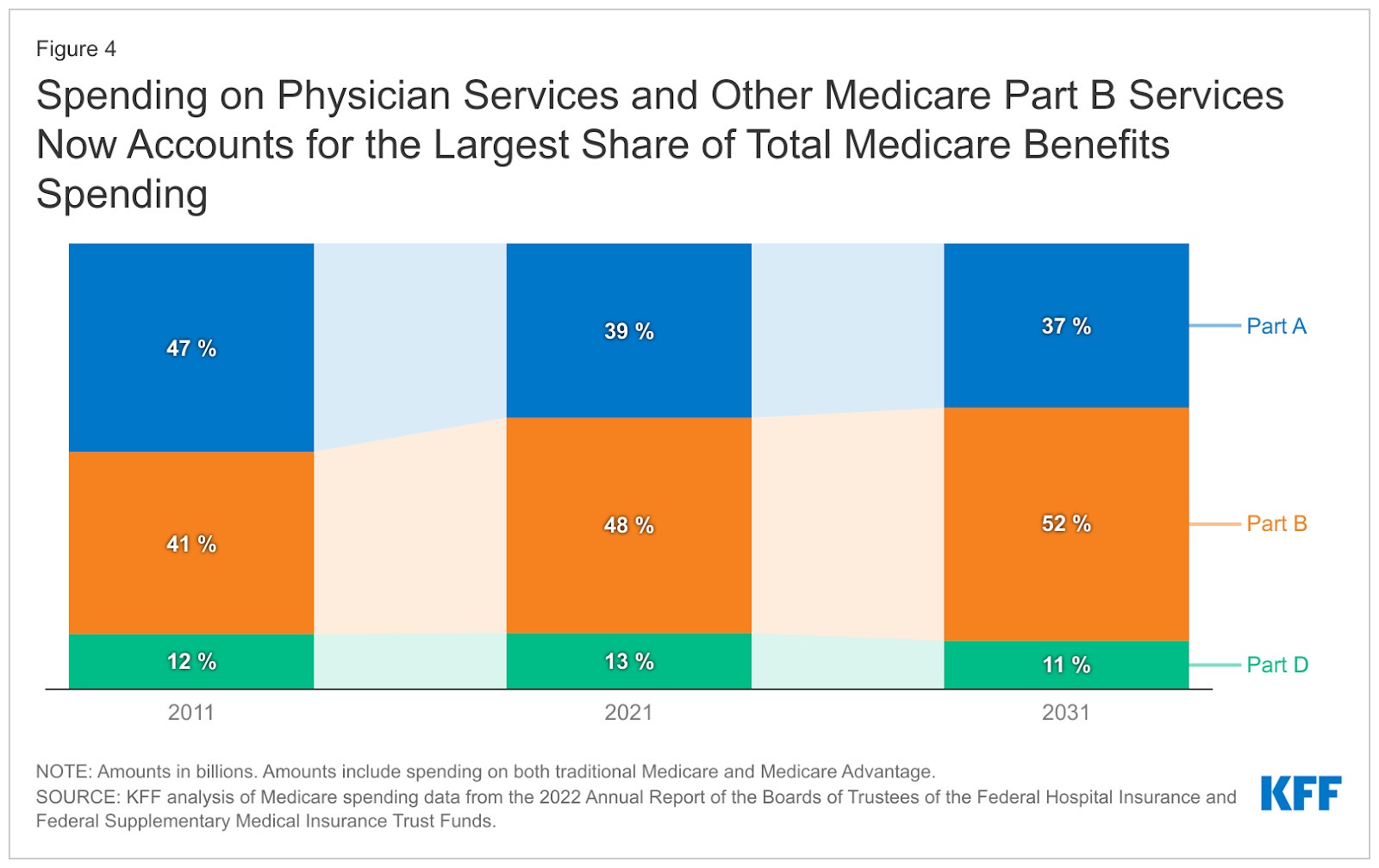
Reining in drug prices has long been the focus of Medicare debate and legislation on Capitol Hill. But drug prices are actually a small and decreasing portion of Medicare spending. A much more pressing cost driver is the size and rapid growth of Medicare spending on physician services, i.e., Medicare Part B. A picture is worth a thousand words.
Medicare Part B pays for outpatient physician services, among other things. It reimburses clinicians on a fee-for-service basis through the Medicare Physician Fee Schedule. This means that the more services are provided, the more money Medicare spends — no matter whether the services are worth the expense and actually doing good to the patients.
Moreover, the Centers for Medicare and Medicaid Services (CMS) sets the prices at the federal level for the entire country (with adjustments reflecting regional differences in the cost of inputs). To do so, they rely on recommendations from a small group of American Medical Association-appointed doctors, most of whom are from specialty societies. The short of it is, specialists tell CMS how much they should be paid. What could go wrong?
Lots. As my colleagues and I detail in a new study:
Prices of complex services keep rising at the expense of primary care services. Because Part B is subject to a budget-neutrality rule, clinicians achieve higher reimbursement rates for specialty services by recommending cuts to primary care services, generally speaking.
The rate differential between primary and specialty services drives up the provision of complex services and drives down the provision of low-reimbursement services.
Providers don’t compete. In the real world, businesses that sell goods and services compete amongst each other by offering the best possible value, i.e., high quality at competitive prices. The MPFS rates aren’t set in a competitive fashion: Instead, when the input costs go up, CMS systematically responds by increasing the reimbursement rates. As a result, prices keep going up and up.
The rising prices of the MPFS lead to cost increases throughout the healthcare system. Most insurance companies use the MPFS as the basis for what they reimburse. When MPFS rates go up, insurance prices go up even more. If you’re trying to understand a core reason for our healthcare cost crisis, look no further.
In sum, Part B drives up prices and spending by design. It can be tweaked, but the bad incentives won’t go away. The best existing alternative to Part B is Part C (Medicare Advantage), because it pays private insurers a flat fee per beneficiary per year that the insurer can use to compensate providers. This encourages competition and efficiency, as insurers have an incentive to make sure that whatever money they spend on a beneficiary’s care is worth it. It’s not a perfect system, and the brief linked below proposes fixes to improve it. But it is the best alternative available right now, in my view.
To go further, please check out the following pieces:
The Hill: Boosting Medicare Advantage can improve healthcare quality and costs (John O’Shea and Kofi Ampaabeng)
Mercatus policy brief: The Medicare Physician Fee Schedule: Overview, Influence on Healthcare Spending, and Policy Options to Fix the Current Payment System (John O’Shea, Elise Amez-Droz and Kofi Ampaabeng)
Sorry, but a lot of this is wrong. You should take a look at Table IV.B6 from the Trustees Report. (https://www.cms.gov/oact/tr/2024)
1. You cite the KFF chart to suggest Medicare spending is driven by physician spending, because you equate Part B spending with physician spending. And then you focus the rest of your post on dynamics in the physician fee schedule. But only ~14% of Part B spending is for services paid under the physician fee schedule.
2. In aggregate, physician fee schedule spending is not really driving any growth in Medicare spending, because it's been basically flat for a decade ($70.6 billion in 2014, $70.9 billion in 2023). That's because all the per-person growth has been offset by the enrollment shift into Medicare Advantage.
3. You suggest we should be concerned with physician spending instead of drug spending, but you're ignoring Part B drugs, which is actually one of the fasting areas of spending growth in Medicare.
4. You say growth in physician spending is driven by price, but actually the overall price level has been growing more slowly than inflation or commercial prices; and it's expected to grow even slower in the future. To the extent that we've had growth in per capita spending for physician services in traditional Medicare, it's been volume + drugs.
5. You say physician spending is growing because specialists just tell CMS how much to pay them. But you're getting confused between how Medicare sets relative prices across services and how Medicare sets the overall price level. The specialists influence relative price levels, but not the overall price level.
6. You suggest the program would save money by shifting more enrollees into Part C, but that's super wrong. The program pays 20%+ more when people switch to Part C.