
It’s Not Just the Private Sector: International Spending Comparisons Reveal High Spending in our Public Healthcare Programs, Too
Governments in the US control more per-capita health spending than most countries spend from public and private sources combined.

You’ve heard it a hundred times: “Despite higher healthcare spending, America’s health outcomes are not any better than those in other developed countries.” Some version of that statement is conveyed in countless news stories and frames many contemporary health policy discussions.
Typically, the not-so-subtle implication is that the US is foolishly refusing to accept a win-win: By adopting a public program of universal health coverage like the rest of the advanced world, we could reduce our health spending and enjoy better health outcomes. The only thing holding us back is our misguided reverence for a private healthcare market that has become bloated and inefficient.
Such reasoning is seductive for its simplicity: The problem is excessive spending, and the culprit is the unbridled market.
I countered that perspective in a post to this blog in June by noting that, when measured in terms of spending, the US healthcare system is no more free market-oriented than those of other high-income countries, including the northern European systems so admired by progressives. In the Netherlands and Finland, for example, a larger share of total health spending is in private hands than in the US.
In this post, rather than analyzing public health spending as a share of total health spending, I’m taking a look at the absolute level of health spending in the US compared to other countries.
Figure 1 compares health spending in the U.S. with a dozen European countries as well as Canada and Japan for 2019, the last year for which updated figures are available. This OECD data breaks per-capita health spending into two categories: “compulsory” spending, which is care directly financed by the government, social insurance, and mandatory private insurance, and “voluntary” spending, including optional private coverage, out-of-pocket expenses, and spending by NGOs and private corporations.
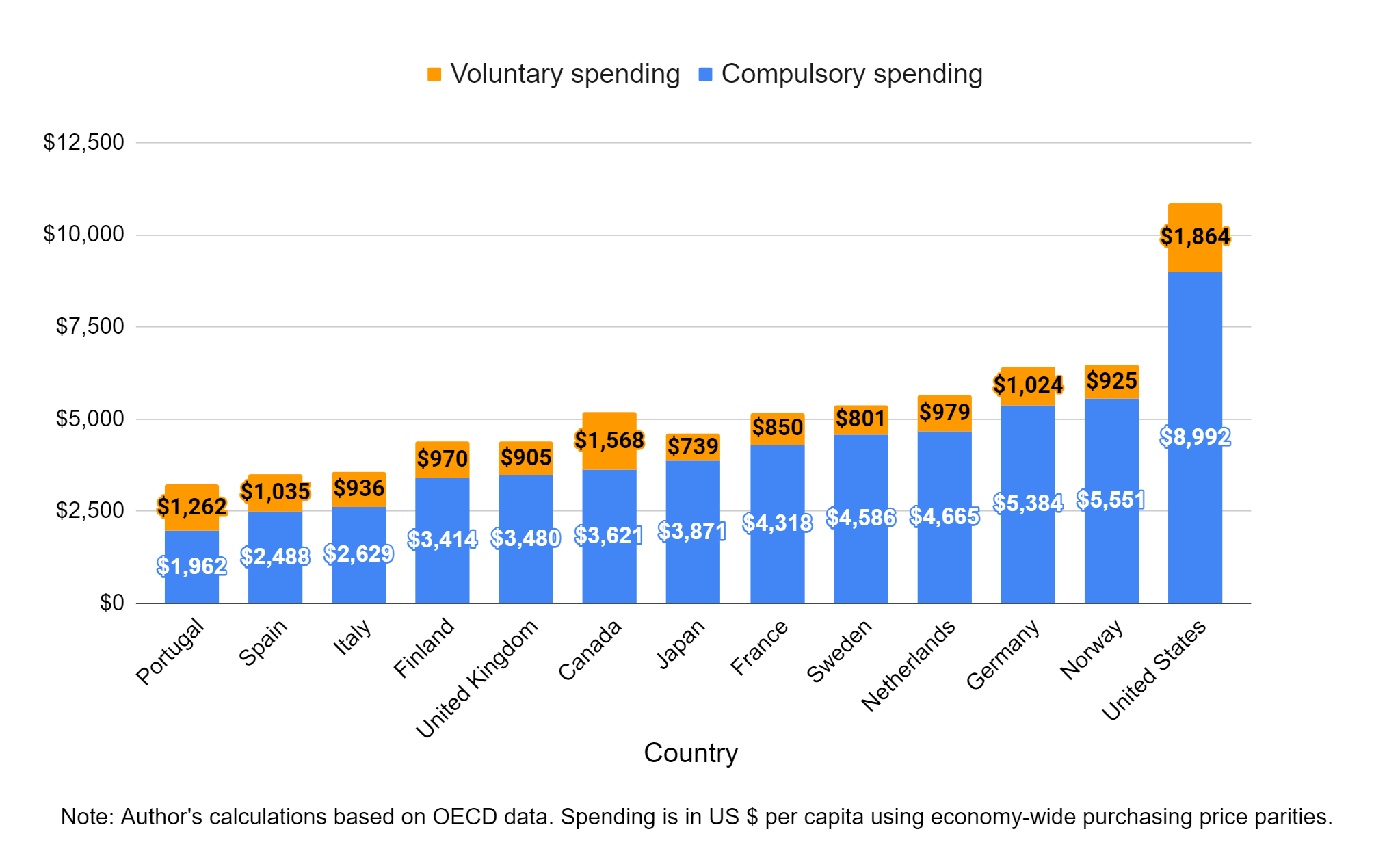
As noted in numerous international comparisons of healthcare financing, total health spending in the US towers above the rest of the world. That much is uncontroversial. But the figure suggests another startling, less discussed fact – that the majority of U.S. health spending is compulsory.
To interpret Figure 1 as a cross-country comparison of public versus private spending, however, would be misleading, due to how the OECD categorizes health spending: Private health insurance in the US, which accounts for one third of our health spending, is considered compulsory due to the individual mandate in the Affordable Care Act.1
This would be akin to classifying the entire US labor market as being under price controls due to the minimum wage. The individual mandate, like the minimum wage, binds on only a small fraction of people. Most people had private health insurance before the individual mandate was adopted, and studies have estimated the mandate increased the number of privately insured individuals by, at most, 12 million – a modest effect considering 220 million Americans had private insurance in 2019. More importantly, though, attributing 2019 health spending to the individual mandate is problematic because the penalties tied to the mandate had already been repealed by then, effectively eliminating the requirement.
A more realistic estimate of compulsory health spending would assign most private insurance – $3,582 per capita by OECD’s reckoning, or one-third of US health spending – to the voluntary column. One could debate what “most” should mean in this context (e.g., it isn’t voluntary to require practicing Catholics to fund a health insurance plan that covers abortions), but to be conservative, I transferred the full amount. That leaves us with $5,446 in per capita voluntary spending and $5,410 in per-capita compulsory spending (Figure 2).

Figure 2 reveals a startling fact: Even after adjusting for the OECD’s inflated compulsory spending in the US, most countries’ total health spending falls below the level of government-controlled (i.e., “compulsory”) health spending in the US.
In other words, if we woke up tomorrow to find private health insurance had been abolished and the 200 million now-uninsured Americans were somehow banned from using their own money on private healthcare, our per-capita health spending would still, amazingly, exceed that of most other advanced countries.
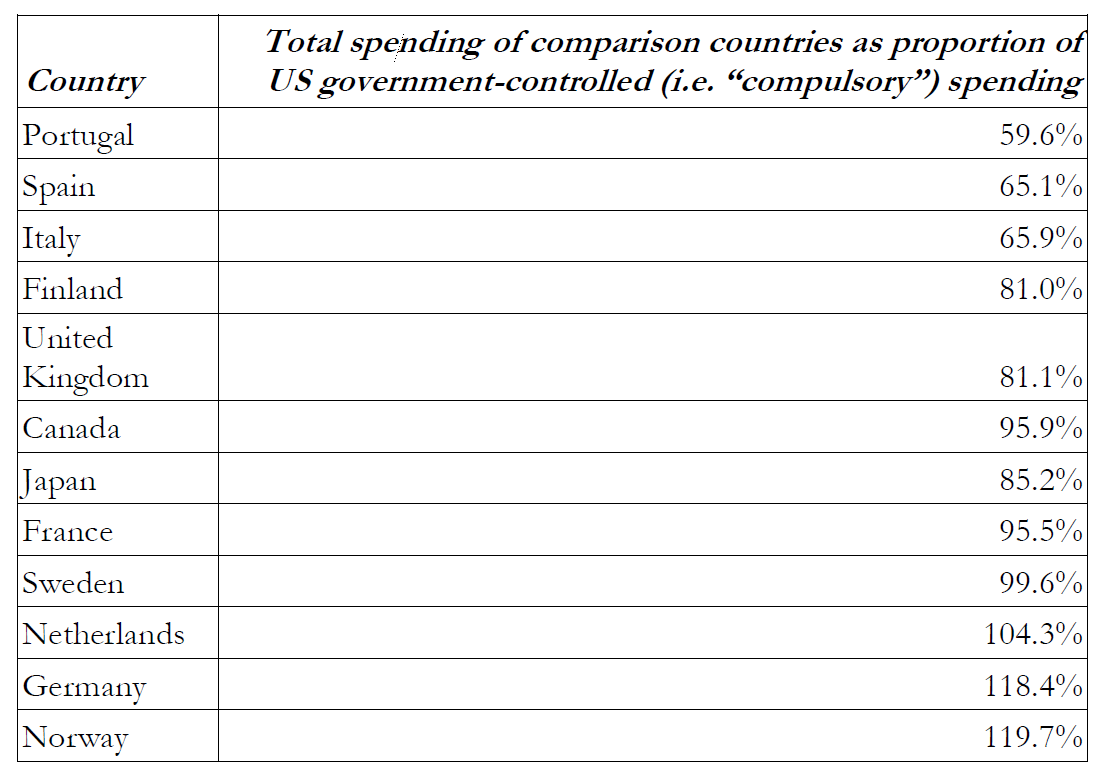
Table 1, derived from the same data as Figure 2, shows how each comparison country measures up. Only three spend more per-capita on their entire health system (compulsory and voluntary spending combined) than the US does on compulsory items alone. The group that spends less includes Canada, the United Kingdom, France, Japan, Finland, and Sweden.
None of this demonstrates that the private healthcare market in the US functions well, or that the government should get out of the business of financing healthcare. But these figures ought to dampen the enthusiasm of those who regard the government as the solution to our healthcare woes. There is no indication that federal and state governments, if given the responsibility to finance all healthcare spending, would do so more efficiently than the current system.
Over the last 70 years, policymakers have permitted Medicaid and Medicare to expand far beyond Congress’ original intent, while at the same time tightening regulation over private insurers, hospitals and providers. US health spending won’t be brought in line with the rest of the world until we’ve grappled with the fact that our public health insurance programs are over-spending and under-delivering.
The OECD is often opaque in describing how it categorizes health spending as compulsory or voluntary. Although the documentation I reviewed didn’t raise any red flags aside from its treatment of US private health insurance spending, it’s possible that additional adjustments could be made to other countries’ figures to improve the accuracy of these comparisons. Therefore, these results should be interpreted as rough estimates and interpreted cautiously.
The OECD is often opaque in describing how it categorizes health spending as compulsory or voluntary. Although the documentation I reviewed didn’t raise any red flags aside from its treatment of US private health insurance spending, it’s possible that additional adjustments could be made to other countries’ figures to improve the accuracy of these comparisons. Therefore, these results should be interpreted as rough estimates and interpreted cautiously.